

L&D nurses are weird. And with that broad generalization, I’ll happily be the first to lay claim to it. As if the very existence of this blog isn’t proof that at the very least, I’m a bit touched, I don’t know what would suffice as evidence.
Happily, in my current job as well as in all previous, I’m far from alone. Unlike in my previous jobs, however, L&D nursing involves a skill that is routinely required and arguably somewhat difficult to master: the art of the cervical exam.
I know I’ve alluded to the complexities of cervical exams in previous posts, but in this one, I’m going to dive into why they’re just so darn difficult at times. I realized as I took place in an admittedly strange but surprisingly commonplace ritual on my unit the other day that cervical exams are something of a low-key hazing for orienting RNs who have little to no OB experience, and that included myself at one time. Abby, one of my new coworkers, was on her way to check her patient who we were trying to determine whether or not to admit for labor, and she was a bit apprehensive as she hadn’t had a whole lot of experience checking women whose cervixes were dilated to less than 5cm.
So as she walked past the desk, the four of us who were there to witness her brave march to triage looked up from our charting, waggled our fingers her way, and gave her our best parting wishes.
So, now that you’ve gotten a look into the oddities of my workplace, let me explain from the very beginning.
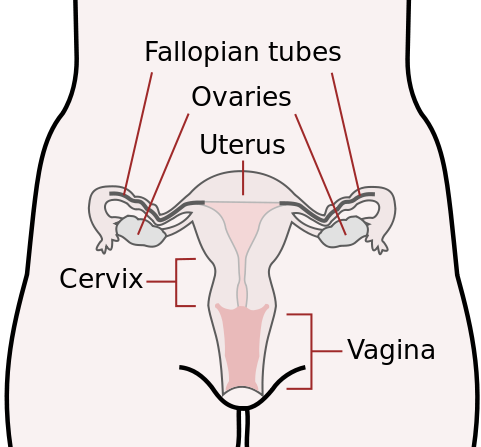
The cervix is a round, muscular ring of tissue that connects the vaginal canal to the uterus. It is essentially the gatekeeper to the womb. In non-pregnant women, the cervix is typically 2-3 cm long. When women become pregnant, the cervix is what allows the sperm to enter the uterus, travel up the fallopian tubes and fertilize the released egg(s).
In a pregnant woman who is not yet in labor or nearing her due date, the cervix should be closed, thick and high in the vaginal canal. As the baby grows, the baby’s presenting part (hopefully the head!) will push the cervix down, and by the 3rd trimester (sometimes even by the 2nd), the cervix should be descended into the vaginal canal far enough that it can be felt by a healthcare provider during a vaginal exam.
Because I need visual representations to really understand things, I found you this picture, courtesy of the CDC:
The Basics of a Cervical Exam
When performing a cervical exam (also called a vaginal exam; these terms are used interchangeably, although the cervix is what you’re looking to assess in both instances), the provider uses the index and middle finger of the dominant hand, inserts those fingers into the vagina, and feels for the cervix.
Especially when you’re starting out, making sure your patient is in a good position before you perform the exam is everything. NOTE: make sure that you make it clear to the patient that you’re going to perform a cervical check and ask her if she wants people to leave the room before you do so! Some women will kick out everyone except you. Others have no problem with having their father, uncles, grandfathers, brothers, and about 20 male cousins all watching as you check. Either way, be sure to ask!
In general, you want your patient to be lying on her back in bed with the head of the bed flat. Have her bring her heels to her butt and let her knees fall out in a butterfly position. Use plenty of gel. No one likes a dry check, and if she’s uncomfortable, she will instinctively scoot back and up the bed, fighting you all the way (this is also known as “climbing the bed” in the vernacular of this particular specialty).
Another trick I’ve learned along the way is to sit on the bed as you perform the exam. This gives you a stable base from which to perform your check, and if you really need to reach for that cervix, it’ll be a lot harder to do it if you’re standing up. You can also keep a hand on her leg that’s nearest you, not only reminding her to stay relaxed, but also as a means of protecting yourself should she kick, either intentionally or reflexively (for the record, I’ve never had this happen, but I fully expect it will and there is nothing wrong with being prepared!).
Especially if she’s young/nervous/sensitive, be sure to talk her through it. Tell her what you’re doing, what she’ll feel and remind her to breathe through any pain she experiences. Be honest with her. If you can’t feel her cervix low in the vaginal canal and you’re going to have to push posterior (toward her back), tell her it will be painful. Encourage her to tell you if she has a history of sexual abuse as this can severely impact how you approach a cervical exam. Don’t be afraid to stop your exam and give her a break if she’s really not tolerating the process well and resume the exam after you’ve both had a chance to take some deep breaths. Some multips have been through so many cervical exams, they don’t really care anymore, but err on the side of caution. Cervical exams are by their very nature uncomfortable and extremely intimate. Be the kind of examiner that you’d want if you had to have your cervix (or your wife/girlfriend’s cervix) checked.
Something to keep in mind (and something that may new L&D nurses struggle with) is that sometimes, no matter how hard you try, cervical exams will hurt your patient. That can be hard to come to terms with as a nurse as we are accustomed to relieving pain, not causing it. This particular exam is incredibly intimate and involves extremely sensitive areas of the female anatomy, which can make it difficult for you as a nurse to carry on when you know your patient is in pain as a direct result of your actions. I promise, you’ll get quicker and more accurate as time goes on, but no matter how good you get, sometimes you won’t be able to avoid causing a bit of pain with cervical checks. Stick to the guidelines in the paragraph above, however, and most patients will still trust you, even after a tough check.
A final piece of advice for this section: when you know the exam is hurting your patient, you can’t talk her through it/apologize afterward too much. And usually both are required to keep her trust after an uncomfortable check.
The First Time You Check A Cervix
The cervix can be tough to find, especially for new L&D nurses because as at first, pretty much everything in there just feels warm and mushy. Most new L&D nurses won’t feel the cervix the first time they perform a vaginal exam. It often takes a few vaginal exams to not only feel comfortable enough to feel around for something that isn’t just vaginal wall, but also to get an idea of what isn’t cervix so that when you do feel one, you know it’s something different. Usually, it takes a few awkward moments of feeling around in there and a near-accidental encounter with a cervix to realize, “oh, that‘s a cervix!”. If you’re new to L&D and struggling with vaginal exams, welcome to the club. There are times where I still can’t find cervixes (especially closed or only slightly dilated ones!) and need to call for a backup checker (typically, the charge nurse).
Standard Deviation: The Art of Cervical Exams
Please note that cervical exams are something of an art. No two cervixes are the same–just like all nurses and doctors are different. So two different people may check the same cervix seconds apart and get different readings. Why? Because there is no way to objectively assess cervical dilation. In all cervical exams, you’re stuck with a subjective manual exam. Sorry, no magical cervical measuring tape here. A cervical exam is based on personal interpretation of one’s own assessment.
So when I check a lady and say she’s a 2 and the next nurse checks and says she’s a 1.5, that may only mean the second nurse has bigger fingers than I do. Really. It can be that arbitrary. Or maybe I checked during a contraction and the next nurse checked between contractions (which is generally the polite thing to do, though early on in labor, your patient may not experience much pain with contractions or feel them at all!). So while cervical exams are certainly an important skill to develop, it is important to keep in mind that they’re not always going to align perfectly from nurse to nurse (or doc to doc or doc to nurse etc.,), though they should at least be in the ballpark of each other. Usually, I’m within 1cm or less of other nurses’/physician’s assessments if there’s any deviation at all. That’s a good goal to strive for.
Cervical Consistency
Depending on dilation and labor stage, cervixes can be hard, medium, or soft in consistency. As cervixes dilate and thin, they also become softer. A hard or moderate cervix can sometimes feel “crinkly” on the edges. A cervix of this consistency typically indicates very, very early labor or a woman who isn’t in labor at all. A soft cervix feels a lot like an earlobe. Usually, you’ll feel a soft cervix in women who are either near their due dates, overdue, or in labor.
What Am I Looking For?
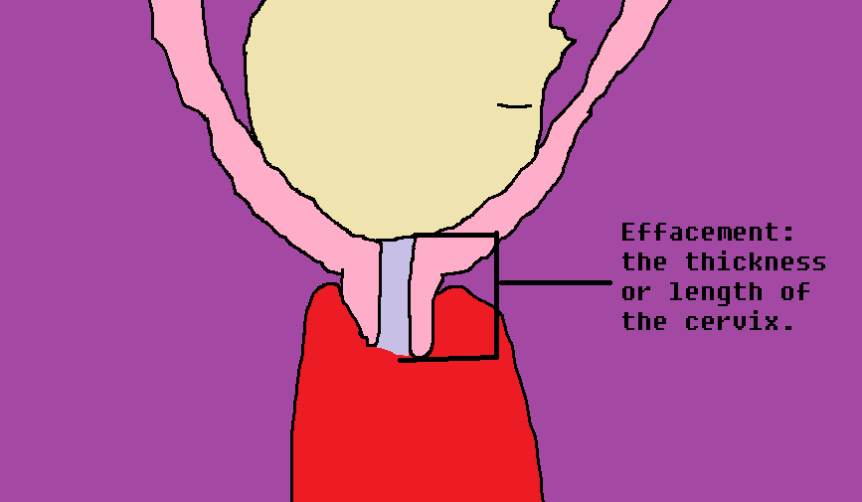
When performing a cervical exam, the nurse is trying to determine if the cervix: 1) has dilated, or opened; 2) has effaced, or thinned out; 3) has a soft vs hard consistency; and 4) is anterior, posterior or centrally located on top of baby’s head.
Dilation
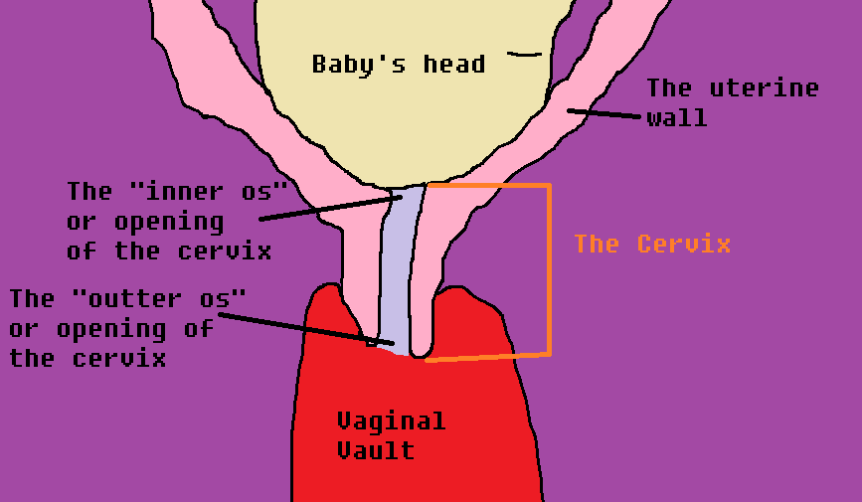
In the diagram above, the light purple section represents the dilation of the cervix. You can see the cervix is somewhat descended into the vaginal vault below, though keep in mind that even in a non-pregnant state, part of the cervix normally protrudes into the vaginal canal. The inner os and outer os are key in determining dilation.

In order to truly determine dilation, you need to be able to reach through the cervix with your finger(s) and touch the baby’s head. The degree of dilation at the inner os is the true dilation of the cervix. Keep that in mind as that has tricked many a newbie before (including me!).
Tip for determining dilation early in your career: take a paper tape measure (the kind used to measure babies) and tape it with the centimeter side up on the back of your name badge. After you check a cervix and discard your glove, use your fingers to check what you felt against the tape measure. This can be a good double-check to see if your assessments are relatively accurate.
Early Stages: Thick, High and Barely Dilated
In a patient who isn’t too far dilated or effaced, a cervix can be not only hard to find, but hard to check. This may be because it is so long that it’s hard to get through to the inner os, or it could be posterior (around the back of the baby’s head) and a long ways away from your curious fingers. A closed cervix usually feels like a dimple and can be really, really difficult to even find.
Personally, I call dilation based on the following:
Fingertip: I can get 1 finger through the cervix, but I can’t quite put it flat on baby’s head at the inner os.
1cm: 1 finger through to the inner os, flat on baby’s head.
2cm: 2 fingers on top of each other through to the inner os on baby’s head.
3cm: 2 fingers side by side through to the inner os on baby’s head.
4cm: 2 fingers through to the inner os, slightly preadable between the edges of the cervix to a degree I can show you on my fingers, but can’t really describe. (This is where your tape measure comes in handy! Figure out what 4cm looks/feels like with your fingers!)
5cm: 2 fingers through to the inner os, spreadable more so than a patient dilated to 4, but less than 6. Again, hard to describe without showing you. Make sure to use your tape measure!
*Your method of determining dilation may be different than mine based on your finger size!
Later Stages: Wide and Thin!
As dilation continues, the cervix will begin to feel less and less like a tube and more and more like a rim around the baby’s head. At a certain point, you will no longer be able to spread your fingers wide enough to determine how dilated your patient is. When this happens, the best method of checking dilation is to find the cervix and to try to put as much of your fingers on it as possible between the edge of the cervix and wall of the vaginal canal. Again, your assessment may vary from mine based on finger size, but my general guidelines are as follows:
6cm: At this dilation, I can usually still spread my fingers enough to perform an adequate exam. However, if I try to put my two fingers on the cervix, there is more cervix than I have finger width.
7cm: I can get 2 fingers side by side on the cervix. *(Remember, 2 fingers side by side is my measurement for 3cm, so if there is this much cervix left, I simply subtract from 10cm to get my dilation. Same goes for the following dilations!).
8cm: I can get 1.5 fingers size by side on the cervix.
9cm: I can get 1 full finger on the cervix. Usually, the cervix feels pretty thin by this point.
9.5cm/lip/rim: a little tiny strip of cervix is still present on your exam. So…close!
10cm: NO CERVIX LEFT! LET’S HAVE A BABY!!!
Effacement
Generally speaking, as a woman’s cervix dilates, it is also going to thin out. So the more dilated a woman is, the thinner her cervix should be. As a woman’s cervix effaces, it lets down the baby’s head into the vaginal vault, so as this progresses, you may notice baby’s head getting lower and lower and that with each check, you have to go in less and less distance to find the head. We measure effacement in percentages in increments of 10 from 0 to 100.
Starting at the thick end, 0% effaced means a woman’s cervix hasn’t thinned out at all. Now, typically, when a cervix is this thick, it’s closed. Unless confirmed by ultrasound, it is fairly unlikely that you will ever be able to insert a finger into a cervix that is 0% effaced, though I’ve felt some that are pretty darn close.
As you might have guessed, 50% effaced is halfway thinned out. On my own assessment, I say that a woman’s cervix is 50% effaced when it comes up to my first knuckle.
From 50% effaced, each increment of 10 brings you a little bit closer to fully effaced, or 100% effaced. Eventually, the cervix may feel so thin and may be so firmly pressed down by baby’s head that it is thin as paper, at which point we’d say the patient is 100% effaced. She just needs to finish dilating and we can think about having a baby!
As you gain experiencing with checking cervixes, you’ll also notice that some cervixes will feel stretchy and you’ll be able to stretch them with your fingers. A stretchy cervix is a happy cervix. This usually means your patient is going to dilate nicely.
It is important to note that in general, first-time moms (primiparas) will undergo more effacement first, then dilation. Mothers who have already had a baby or babies (multiparas) tend to dilate more, then efface. So if you check a primipara who is in labor and you note her cervix is extremely thin, and then on your second check, you can’t find it, slow down, retrace your steps, and check again. I’ve had patients who have been fully effaced at a dilation of 3. Those cervixes are darn near impossible to find, but typically, you can if you’re thorough!
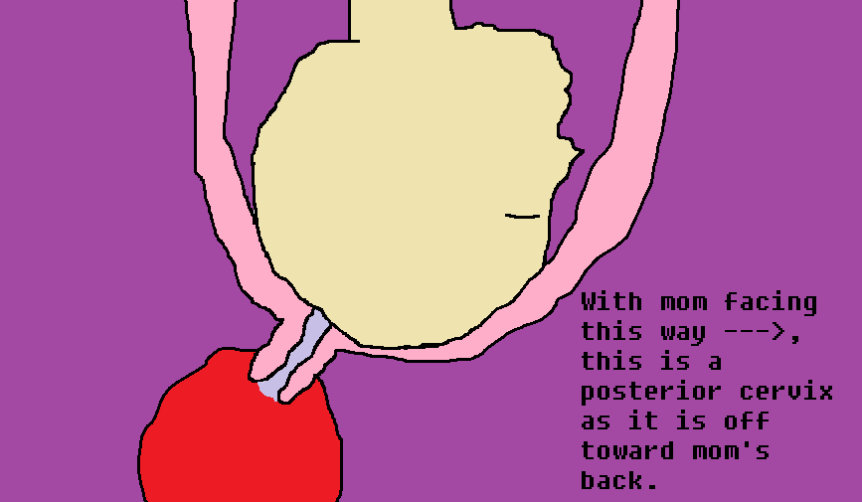
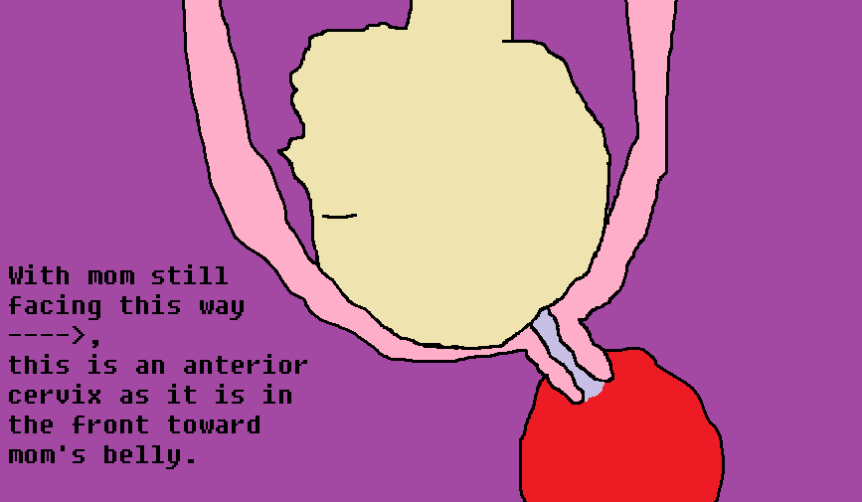
Cervical Position
As I’ve referenced above, cervixes aren’t always straight back. Sometimes, especially in a mom who isn’t too far dilated and isn’t really ready for labor, her cervix will be posterior, or to the back of the vaginal vault. Some cervixes are very anterior, or toward the front of baby’s head, and they sit “up”, just past the pubic bone. Some cervixes are off to the sides.
The truly wonderful ones, however, are in mid-position (straight back), soft, and consistently dilating/effacing in an effort to bring us a baby.
Station
Although station isn’t related to the position of the cervix, this is also something you’ll be paying attention to when you check your patient.
As you check mom’s dilation and effacement, take note of where the top of baby’s head (again, presenting part, so hopefully the head!) is in relation to the ischial spines (bony prominences of the pelvis that are in the narrowest area of the vaginal vault) . Even if you have to go way back to find mom’s cervix, the baby’s head may be low in the vaginal vault, and where the front-most part of baby’s head is in relation to the pubic bone determines station.
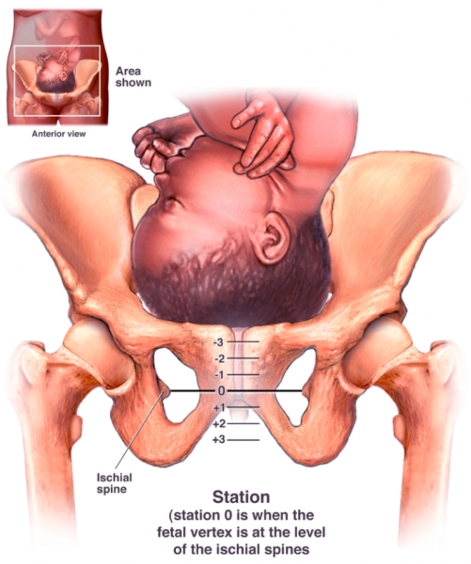
In terms of station, the baby’s head is said to be fully engaged when he reaches 0 station. By the time baby is at 3+ station, the head is crowning. Typically, by the time baby reaches 1+ station, the head may be just visible when mom pushes with contractions.
Tricks for Cervical Exams
A good trick to check a minimally dilated cervix or any woman who you are checking for the first time is to use your middle finger (or longest finger) to sweep along the baby’s head, starting anteriorly (toward the front) and going back. Don’t forget to check the sides!
For minimally dilated cervixes that are too far back to reach: when you find the edge of the cervix, hook it with your middle finger and pull it gently down toward you. Usually, you can insert your second finger at this time and get a good feel for dilation and effacement.
Another tip is to have your patient make a fist and put it underneath the small of her back. This can help to tip the cervix forward in the vaginal vault so it’s easier to reach.
If baby’s head is not engaged in the pelvis, sometimes pushing down gently on mom’s belly can bring a floating baby down, therefore pushing the cervix toward you.
Most of all, be patient and don’t be afraid to have someone check after you, just to make sure!
Happy cervical exams, fellow L&D nurses! May the cervix be with you!
Reading from Reddit? Read CervixWithASmile’s reply to comments here!

This is the best thing ever!!
LikeLike
When you are doing your 7-10cm and you say you do 2 fingers side by side and subtract and so on, what exactly are you doing/measuring with your fingers? I know how to find a cervix (sometimes – I’m still learning) when I can put my fingers in and find the whole ring, but I just can’t visualize when you can’t spread your fingers across what you are measuring to subtract by. Can you explain? Thanks!
LikeLike
Hi Lisa, sure! Let me try to explain better. When you can no longer spread your fingers, you have to find the cervix itself and use your finger widths to measure the amount of cervix remaining. So what you’re measuring is the cervix itself, not the space between the sides. I hope that helps!
LikeLike